
After watching your two videos on fascia iliaca blocks, I started using them with pretty good success for hip arthroscopies. Today I used one for a total hip arthroplasty. The patient was a 60 y/o female with a bit of a belly hanging over her inguinal area. Using Dr. HIckmans's technique, I injected 50 mls of 0.25% Bupiv with a splash of epi. By the end of the block, she said her hip was painless for the first time in years. During surgery, I ran her on 3% Des plus occasional bumps of ephedrine and neo to maintain her BP above 80. I gave her no narcotics. In the PACU, she was wide awake and joking with the nurses, pain score was 0/10. I went to see her this evening and she had been up ambulating and was still pain free. Next time, I'll try inserting a catheter.
we love this technique at our place, we place fascia iliaca catheters for all of our hip fractures.
Thanks for the case feedback. I am glad to hear the techniques are proving to be useful. I love hearing stories about patient comfort facilitated by regional anesthesia. Keep up the great work!
That is awesome. I am so happy it is working for you all. Isn't it so rewarding to see a patient like that in the PACU?
It is awesome, because all of my partners and all but one of my surgeons believe that the only anesthetic technique for total hips and knees is a spinal. I love proving that I can deliver pain free patients who can still ambulate within hours of surgery without having a spinal (and hence without need of a Foley.) The floor nurses say my patients have awesome recoveries.
These days in anesthesia, one gets their rewards in unexpected places.
Was wondering if this block delivers anterior knee analgesia as well. The femoral n. is blocked in this approach too?
The femoral nerve is definitely blocked with this approach so it would cover that part of the knee. You are also blocking the obturator nerve which in some cases innervates the medial knee and can be a factor. I have not heard of anyone using an FIB for knee surgery but I guess you could. Obviously there will be significant motor weakness so appropriate precautions should be made. We utilize patient education and a straight leg brace. Most folks stick to femorals or adductor canal blocks and catheters for knee surgery.
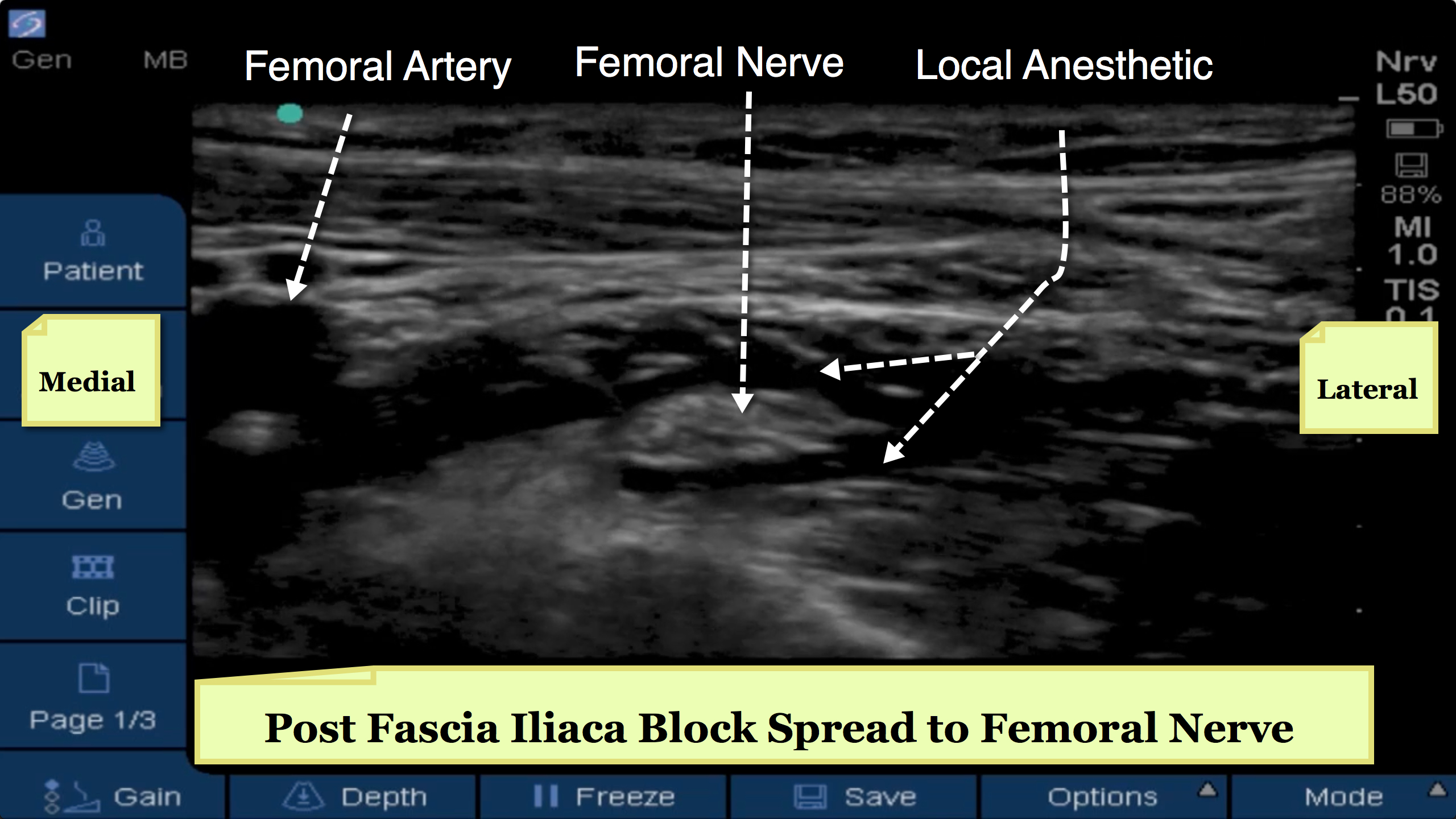
I concur with Dr. Hickman. Here is an annotated screenshot of the femoral nerve totally surrounded by local anesthetic after a fascia iliaca block.
Thanks for the confirmation. How do you all minimze the motor weakness then after a FIB? Is the main consideration LA concentration? I am thinking of hip procedures mainly.
LA concentration and time after the block to let it resolve. I am not aware of anyway to avoid the motor weakness. Someone stated above their patient was walking the evening of surgery. I would be VERY careful trying to do that. Different patients obviously respond differently.
I would not encourage ambulation the same day of a solid FIB block.
anterior inferior illiac spine(AIIS) is the land mark .but is difficult to visualise as it is deeper than ASIS.AIIS lies exactly below the the fascia illiaca where you have to deposit the local medication ie internal oblique and sartorius